
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
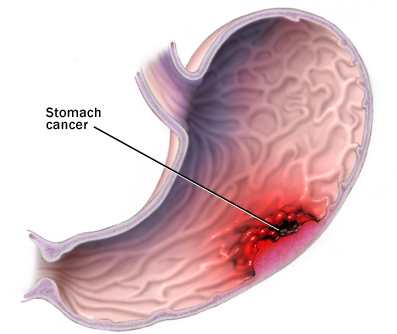
Stomach Cancer
Gastric cancer, commonly referred to as stomach cancer, can develop in any part of the stomach and may spread throughout the stomach and to other organs; particularly the esophagus, lungs, lymph nodes, and the liver. Stomach cancer causes about 800,000 deaths worldwide per year.
Stomach cancer is often asymptomatic or causes only nonspecific symptoms in its early stages. By the time symptoms occur, the cancer has often reached an advanced stage (see below), one of the main reasons for its poor prognosis.
Stomach cancer can cause the following signs and symptoms:
Stage 1 (Early)
- Indigestion or a burning sensation (heartburn)
- Loss of appetite, especially for meat
- Abdominal discomfort or irritation
Stage 2 (Middle)
- Weakness and fatigue
- Bloating of the stomach, usually after meals
Stage 3 (Late)
- Abdominal pain in the upper abdomen
- Nausea and occasional vomiting
- Diarrhea or constipation
- Weight loss
- Bleeding (vomiting blood or having blood in the stool) which will appear as black. This can lead to anemia.
- Dysphagia; this feature suggests a tumor in the cardia or extension of the gastric tumor in to the esophagus.
 Note that these can be symptoms of other problems such as a stomach virus, gastric ulcer or tropical sprue. Diagnosis should be done by a gastroenterologist or an oncologist.
Note that these can be symptoms of other problems such as a stomach virus, gastric ulcer or tropical sprue. Diagnosis should be done by a gastroenterologist or an oncologist.
Causes
Infection by Helicobacter pylori is believed to be the cause of most stomach cancer while autoimmune atrophic gastritis, intestinal metaplasia and various genetic factors are associated with increased risk levels. The Merck Manual states that diet plays no role in the genesis of stomach cancer. However, the American Cancer Society lists the following dietary risks, and protective factors, for stomach cancer: "smoked foods, salted fish and meat, and pickled vegetables (appear to increase the risk of stomach cancer.)
Nitrates and nitrites are substances commonly found in cured meats. They can be converted by certain bacteria, such as H. pylori, into compounds that have been found to cause stomach cancer in animals. On the other hand, eating fresh fruits and vegetables that contain antioxidant vitamins (such as A and C) appears to lower the risk of stomach cancer." A December 2009 article in American Journal of Clinical Nutrition found a statistically significant inverse correlation between higher adherence to a Mediterranean Dietary Pattern and stomach cancer.
In more detail, H. pylori is the main risk factor in 65-80% of gastric cancers, but in only 2% of such infections. Approximately ten percent of cases show a genetic component.
In Japan and other countries bracken consumption and spores are correlated with incidence of stomach cancer, though causality has yet to be established.
A very important but preventable cause of gastric cancer is tobacco smoking. Smoking increases the risk of developing gastric cancer considerably; from 40% increased risk for current smokers to 82% increase for heavy smokers which is nearly twice the risk for non-smoking population.
Gastric cancers due to smoking mostly occur in upper part of stomach near esophagus Another lifestyle cause of gastric cancer besides smoking is consumption of alcohol. Alcohol as cause of cancer along with tobacco smoking as cause of cancer increase the risk of developing other cancers as well.
Gastric cancer shows a male predominance in its incidence as up to three males are affected for every female. Estrogen may protect women against the development of this cancer form. A very small percentage of diffuse-type gastric cancers (see Histopathology below) are thought to be genetic. Hereditary Diffuse Gastric Cancer (HDGC) has recently been identified and research is ongoing.
However, genetic testing and treatment options are already available for families at risk.
Some researchers showed a correlation between Iodine deficiency or excess, iodine-deficient goitre and gastric cancer; a decrease of the incidence of death rate from stomach cancer after implementation of the effective I-prophylaxis was reported too. The proposed mechanism of action is that iodide ion can function in gastric mucosa as an antioxidant reducing species that can detoxify poisonous reactive oxygen species, such as hydrogen peroxide.
Diagnosis
To find the cause of symptoms, the doctor asks about the patient's medical history, does a physical exam, and may order laboratory studies. The patient may also have one or all of the following exams:
- Gastroscopic exam is the diagnostic method of choice. This involves insertion of a fiber optic camera into the stomach to visualize it.
- Upper GI series (may be called barium roentgenogram)
- Computed tomography or CT scanning of the abdomen may reveal gastric cancer, but is more useful to determine invasion into adjacent tissues, or the presence of spread to local lymph nodes.
Abnormal tissue seen in a gastroscope examination will be biopsied by the surgeon or gastroenterologist. This tissue is then sent to a pathologist for histological examination under a microscope to check for the presence of cancerous cells. A biopsy, with subsequent histological analysis, is the only sure way to confirm the presence of cancer cells.
Various gastroscopic modalities have been developed to increased yield of detect mucosa with a dye that accentuates the cell structure and can identify areas of dysplasia. Endocytoscopy involves ultra-high magnification to visualize cellular structure to better determine areas of dysplasia. Other gastroscopic modalities such as optical coherence tomography are also being tested investigationally for similar applications.
A number of cutaneous conditions are associated with gastric cancer. A condition of darkened hyperplasia of the skin, frequently of the axilla and groin, known as acanthosis nigricans, is associated with intra-abdominal cancers such as gastric cancer. Other cutaneous manifestations of gastric cancer include tripe palms (a similar darkening hyperplasia of the skin of the palms) and the sign of Leser-Trelat, which is the rapid development of skin lesions known as seborrheic keratoses.
Various blood tests may be done; including: Complete Blood Count (CBC) to check for anemia. Also, a stool test may be performed to check for blood in the stool.
Staging
If cancer cells are found in the tissue sample, the next step is to stage, or find out the extent of the disease. Various tests determine whether the cancer has spread and, if so, what parts of the body are affected. Because stomach cancer can spread to the liver, the pancreas, and other organs near the stomach as well as to the lungs, the doctor may order a CT scan, a PET scan, an endoscopic ultrasound exam, or other tests to check these areas. Blood tests for tumor markers, such as carcinoembryonic antigen (CEA) and carbohydrate antigen (CA) may be ordered, as their levels correlate to extent of metastasis, especially to the liver, and the cure rate.
Staging may not be complete until after surgery. The surgeon removes nearby lymph nodes and possibly samples of tissue from other areas in the abdomen for examination by a pathologist.
The clinical stages of stomach cancer are:
- Stage 0. Limited to the inner lining of the stomach. Treatable by endoscopic mucosal resection when found very early (in routine screenings); otherwise by gastrectomy and lymphadenectomy without need for chemotherapy or radiation.
- Stage I. Penetration to the second or third layers of the stomach (Stage 1A) or to the second layer and nearby lymph nodes (Stage 1B). Stage 1A is treated by surgery, including removal of the omentum. Stage 1B may be treated with chemotherapy (5-fluorouracil) and radiation therapy.
- Stage II. Penetration to the second layer and more distant lymph nodes, or the third layer and only nearby lymph nodes, or all four layers but not the lymph nodes. Treated as for Stage I, sometimes with additional neoadjuvant chemotherapy.
- Stage III. Penetration to the third layer and more distant lymph nodes, or penetration to the fourth layer and either nearby tissues or nearby or more distant lymph nodes. Treated as for Stage II; a cure is still possible in some cases.
- Stage IV. Cancer has spread to nearby tissues and more distant lymph nodes, or has metastatized to other organs. A cure is very rarely possible at this stage. Some other techniques to prolong life or improve symptoms are used, including laser treatment, surgery, and/or stents to keep the digestive tract open, and chemotherapy by drugs such as 5-fluorouracil, cisplatin, epirubicin, etoposide, docetaxel, oxaliplatin, capecitabine, or irinotecan.